
Kenya Advances Public Health Emergency Response Systems through Validation of a Risk-Based Decision-Making Tool

Kenya’s States Parties Self-Assessment Annual Reporting (SPAR 2025) signals a strategic shift in Health Security Preparedness
February 13, 2026
What the U.S “Advancing Global Health” Initiative Means for Africa’s Health Security and Sovereignty
March 10, 2026
From Ad Hoc Response to Structured Activation: Operationalizing a Standardized Escalation Framework to Improve Speed, Clarity, and Accountability in Emergency Response
Feb 19 -20, 2026, Nairobi-Kenya
The Center for Global Health and Pandemic Intelligence (CGP) in collaboration with the Kenya National Public Health Institute (KNPHI), with support from Tackling Deadly Diseases Programme (TDDAP2) provided technical leadership in the National Validation Workshop for the Decision-Making Tool for Public Health Emergencies (DMT-PHE) training curriculum. This milestone represents a significant advancement in Kenya’s public health emergency governance and reinforces the country’s compliance with the International Health Regulations (IHR 2005)
From Framework Validation to Institutionalized Risk-based Activation
The curriculum validation marked the institutionalization phase of DMT-PHE transitioning from framework validation (October 2025) to applied national rollout readiness. Table Top Simulations (TTX) across five high-risk scenarios—Public Health Event of Unknown Etiology (PHEIUE), Rift Valley Fever (RVF), Ebola, Chemical Spill, and Cholera, tested classification logic, escalation thresholds, and IMS activation under time pressure.The exercises were aligned to Kenya’s PHEM framework, ERF IMS framework, IDSR workflows, Event-Based Surveillance systems, 7-1-7 timeliness benchmarks, and the risk-assessment decision instrument under Annex 2 of the IHR (2005).

Embedding IHR Annex 2 into Decision Logic
Annex 2 of the IHR (2005) requires States Parties to notify WHO of events that may constitute a Public Health Emergency of International Concern (PHEIC) based on structured risk assessment.
Through simulations, participants applied:
- “Serious” and “Unusual” criteria
- Automatic notifiable condition logic (e.g., VHF/Ebola)
- Cross-border notification triggers
- Threshold-based escalation for epidemic-prone diseases
- Conditional notification for non-infectious hazards
Escalation was tested under uncertainty, reinforcing that timely notification is a preventive risk-management decision not a post-confirmation action.
Operationalizing One Health in Real Time
The validation embedded One Health into the decision-making logic. It operationalized multisectoral escalation in real-time simulation, ensuring that animal health signals, environmental hazards, and human health alerts were integrated into unified escalation pathways. Scenarios reflected Kenya’s real epidemiological landscape, including livestock mobility corridors, environmental basin connectivity, and cross-border exposure dynamics
Validation Results
Evaluation findings confirmed strong endorsement:
- 45 national and county reviewers participated
- Average workshop rating: 4.56 / 5
- 96% confirmed readiness for piloting and rollout (with minor refinements)
- Strong agreement on alignment with PHEM, IMS, IDSR, One Health, and IHR (2005) Annex 2 criteria
The validation confirmed that DMT-PHE strengthens existing surveillance systems while reducing decision latency during escalation.
“The simulations clarified escalation thresholds and strengthened our confidence in applying Annex 2 risk assessment under uncertainty. The integration with IDSR, IMS structures, PHEM, and ADaM platform makes the tool practical for county-level implementation.” James Mbugua, County Disease Surveillance Coordinator, Lamu County

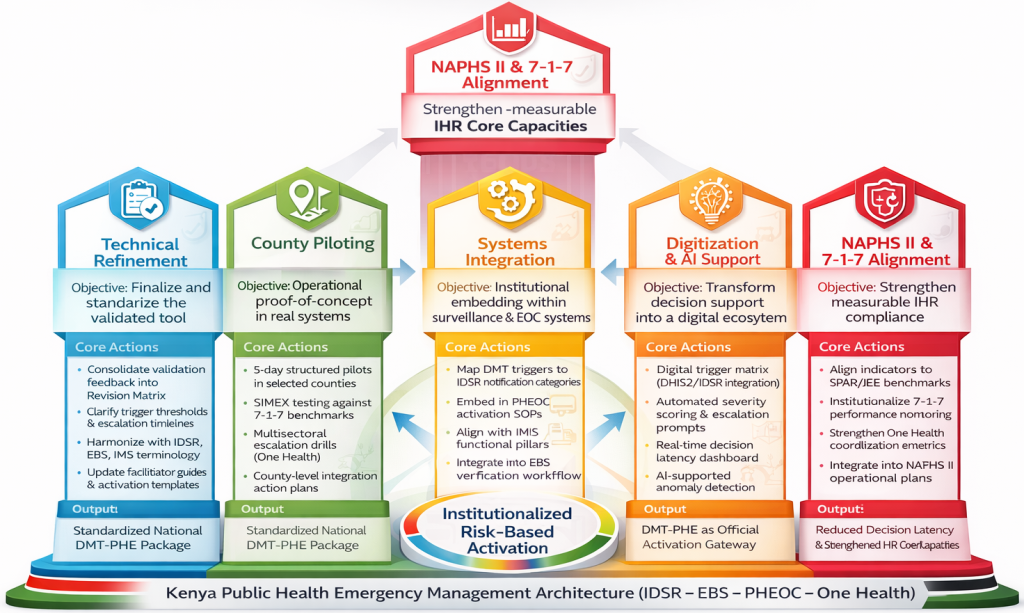
Envisioned DMT Implementation Pathway (2026-2028)
Pillar 1 – Technical Refinement focuses on consolidating validation feedback into a standardized Version 2.0 of the tool. This includes clarifying trigger thresholds and escalation timelines, harmonizing terminology with IDSR, EBS, and Incident Management System (IMS) standards, and updating facilitator guides and activation templates. The result is a nationally standardized DMT-PHE package.
Pillar 2 – County Piloting tests operational feasibility in selected counties through structured 5-day pilots. Simulation exercises benchmark performance against 7-1-7 targets, assess multisectoral escalation (One Health), and generate county-level integration action plans. Lessons inform national scale-up.
Pillar 3 – Systems Integration embeds DMT-PHE within routine surveillance and emergency workflows. Triggers are mapped to IDSR notification categories, integrated into PHEOC activation SOPs, aligned with IMS functional pillars, and linked to EBS verification processes. This establishes DMT-PHE as the official activation gateway.
Pillar 4 – Digitization & AI Support advances digital trigger matrices within DHIS2/IDSR platforms, introduces automated severity scoring and escalation prompts, enables real-time dashboards for decision latency monitoring, and applies AI-supported anomaly detection. This transforms the tool into a dynamic decision-support system.
Pillar 5 – NAPHS II & 7-1-7 Alignment strengthens measurable compliance with IHR core capacities. The framework aligns indicators to SPAR/JEE benchmarks, institutionalizes 7-1-7 performance monitoring, reinforces One Health coordination metrics, and integrates DMT-PHE into NAPHS II operational plans.
Together, these pillars institutionalize risk-based activation within Kenya’s Public Health Emergency Management architecture (IDSR–EBS–PHEOC–One Health), reducing decision latency and strengthening national preparedness.
Regional Preparedness Implications
Kenya’s geographic position within East Africa necessitates strong cross-border notification discipline. By embedding Annex 2 logic and cross-border escalation triggers into structured workflows, the DMT-PHE enhances Kenya’s contribution to regional outbreak containment and continental health security resilience.
Strengthening Global Health Security
The validation of the DMT-PHE curriculum signals Kenya’s commitment to structured, risk-based escalation governance aligned with IHR (2005) obligations and regional preparedness priorities. CGP remains committed to supporting KNPHI and multisector partners in institutionalizing evidence-based decision systems that protect communities and strengthen global health security.

The validation workshop convened representatives from the Kenya National Public Health Institute, Ministry of Health, Africa Centres for Disease Control and Prevention, US CDC, Palladium, Washington State University, Kenya Institute of Primate Research, Directorate of Veterinary Services, Ministry of Environment and Forestry, Kenya Red Cross Society, Amref Health Africa, WHO, Kenya Medical Research Institute, FHI 360, PATH, and county health departments from Nairobi, Kisumu, Murang’a, Lamu, Mombasa, and Uasin Gishu.
This multisector participation reinforced national ownership and ensured subnational realities informed the validation process.






















{kind=link}