
Operationalizing 7-1-7 : Kenya’s shift from metrics and timelines to Decision Intelligence

Kenya Launches NAPHS II and KNPHI Strategic Plan to Strengthen Epidemic Intelligence and Digital Public Health Systems
March 28, 2026
Kenya and the Future of Global Health Security: Balancing Sovereignty, Preparedness, and Solidarity in the Wake of the Ebola Outbreak
May 29, 2026
Dr. Mark Nanyingi | Nairobi-Kenya| April 11 2026- 00:00
Designing systems that deliver speed in outbreak response
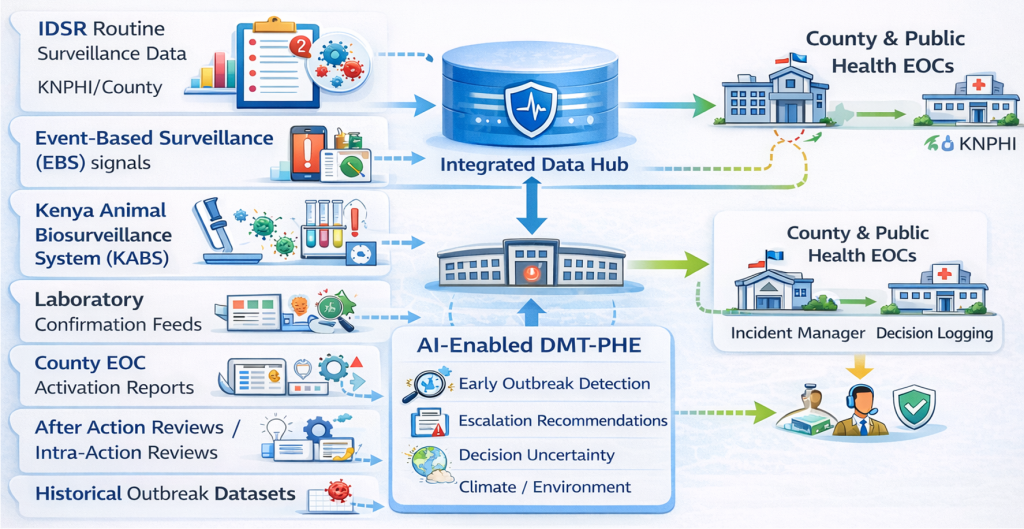
The Kenya National Public Health Institute (KNPHI), supported by the African Field Epidemiology Network (AFENET) and with technical guidance from the Center for Global Health and Pandemic Intelligence (CGP), convened a national workshop to operationalize 7-1-7. The emphasis was not on introducing the framework, but on interrogating its application. Through simulation exercises, early action reviews, and hands-on engagement with national dashboards, participants explored how decisions are made in real time and where delays emerge. A key innovation within this process was the pilot integration of AI-assisted decision support within the Decision-Making Tool for Public Health Emergencies (DMT-PHE), marking a shift toward embedding intelligence directly into operational workflows.

Why 7-1-7
While the framework defines what should happen and when, it does not fully address how those timelines are operationalized within complex, decentralized health systems. Increasingly, evidence suggests that the limiting factor is not the absence of surveillance but the absence of structured decision-making systems that translate signals into timely action.ties.
The 7-1-7 framework has rapidly become a cornerstone of global health security, setting clear expectations for how quickly outbreaks should be detected, notified, and responded to. At its core, 7-1-7 defines three critical timelines: detection of a public health event within 7 days of emergence, notification to relevant authorities within 1 day, and initiation of an effective response within 7 days. These benchmarks have strengthened accountability, sharpened performance measurement, and provided a common language for timeliness across countries. By translating complex outbreak response processes into measurable intervals, 7-1-7 enables systems to assess not just whether they respond—but how fast they do so. Yet an important question persists across many settings:
How do we consistently achieve these timelines in real-world conditions?
While the framework defines what should happen and when, it does not fully address how those timelines are operationalized within complex, decentralized health systems. Increasingly, evidence suggests that the limiting factor is not the absence of surveillance but the absence of structured decision-making systems that translate signals into timely action.
Where Timeliness Breaks Down
Across multiple country contexts, a consistent pattern is emerging. Surveillance systems are improving. Signals are detected earlier. Data flows are expanding across routine reporting, event-based surveillance, and community intelligence. However, delays persist—not at the point of detection, but in the transition from signal to action. Uncertainty in risk classification, hesitation in escalation, and fragmentation in coordination create what can be described as decision latency. These delays are often subtle, but cumulatively they undermine the ability to meet 7-1-7 targets.
“The challenge is no longer seeing the signal, it is deciding what to do, when, and how. Operationalizing 7-1-7 requires more than the timelines; it requires systems that translate signals into coordinated action,” Dr. Nanyingi

The Missing Layer: Decision Intelligence
At the center of Kenya’s approach is the recognition that outbreak response is fundamentally a decision process. The DMT-PHE provides a structured decision layer that connects detection to response. It systematically converts signals into risk classifications, links those classifications to escalation thresholds, and maps them to predefined response actions. In doing so, it replaces variability with consistency and ambiguity with clarity. Without such systems, response decisions are often shaped by individual experience, institutional memory, or situational judgment. While these elements remain important, they introduce variability and delay.With structured decision pathways, the system itself guides action ensuring that similar signals trigger similar responses, regardless of location or personnel. Surveillance detects events. Decision systems determine response speed.
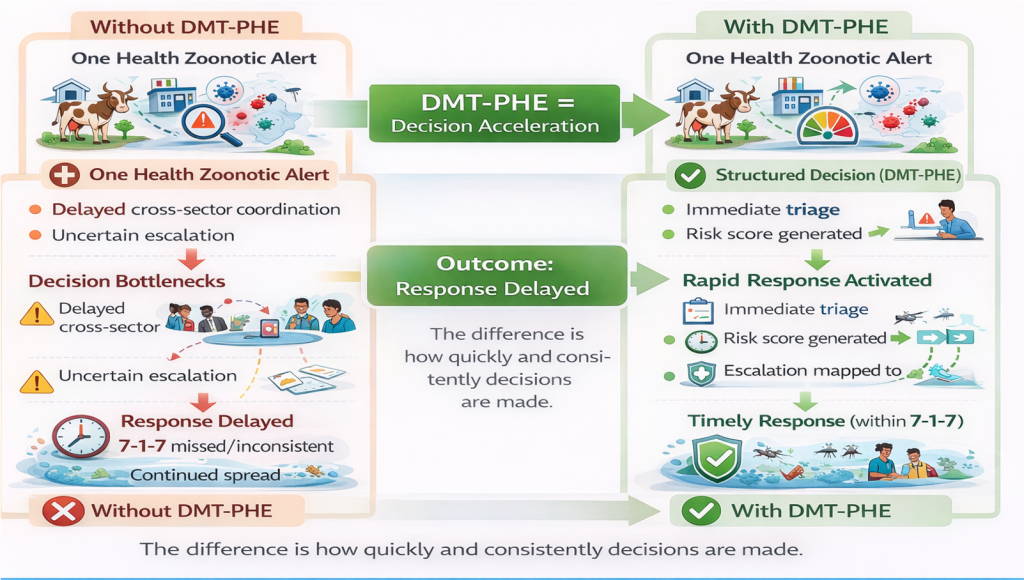
Speed and Structure: A Complementary System
Understanding the relationship between 7-1-7 and decision systems is critical. 7-1-7 defines the speed of the system. It establishes the outer limits within which action must occur.
DMT-PHE defines the structure of the system. It determines how decisions are made within that timeframe.Together, they form a complete operational model:Speed without structure leads to inconsistency. Structure without speed leads to delayed response.
The Role of Artificial Intelligence
The integration of AI into this framework introduces a new dimension of capability. By supporting rapid triage, pattern recognition, and consistency in classification, AI enhances the system’s ability to process signals at scale while reducing cognitive burden on frontline responders. Rather than replacing human judgment, AI acts as an augmenting layer, strengthening the reliability and speed of decision-making in high-pressure environments. This is particularly relevant in decentralized systems, where variability in experience and capacity can affect response consistency. Timeliness is not achieved by urgency it is achieved by design.”
A One Health Imperative
Outbreaks are increasingly shaped by complex interactions across human, animal, and environmental systems. Signals often emerge simultaneously across these domains, requiring integrated interpretation and coordinated response. Kenya’s operationalization of 7-1-7 reflects a One Health approach, ensuring that decision systems are capable of synthesizing multisectoral inputs and triggering cross-sectoral action. This integration is essential not only for zoonotic diseases, but also for climate-sensitive health threats, where early warning depends on linking environmental and epidemiological data.
From Reporting to Performance, and Designing for Speed
A central risk in the global adoption of 7-1-7 is that it becomes a tool for reporting rather than a mechanism for performance improvement.In such scenarios, delays are documented with increasing precision—but not necessarily reduced.Kenya’s approach offers a different trajectory. By embedding 7-1-7 within decision systems, the framework evolves from a passive metric to an active driver of response. Ultimately, achieving timely outbreak response requires intentional system design. Systems must define thresholds clearly, standardize escalation pathways, integrate data across sectors, and provide decision support to those responsible for action. Speed is not an emergent property it is an engineered outcome.
From Timelines to Action
As global health systems continue to strengthen preparedness and response, the next frontier lies not in defining better metrics, but in embedding those metrics into operational systems that enable real-time decision-making. Health security is ultimately a decision problem—and better decisions are the foundation of faster response. Kenya’s experience demonstrates that when surveillance, decision intelligence, and response systems are aligned, performance is no longer aspirational—it becomes achievable.





















{kind=link}